
 The knee joint is buffered by a layer of articular cartilage that caps the ends of the femur (thigh bone) and tibia (shin bone). Another cartilage component, called the meniscus, forms an extra cushion where the leg bones meet to form the knee joint — like a wedged shock absorber that helps distribute weight evenly in the knee.
The knee joint is buffered by a layer of articular cartilage that caps the ends of the femur (thigh bone) and tibia (shin bone). Another cartilage component, called the meniscus, forms an extra cushion where the leg bones meet to form the knee joint — like a wedged shock absorber that helps distribute weight evenly in the knee.
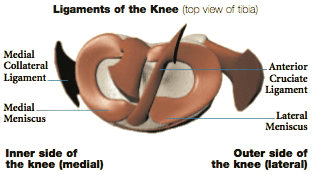
The meniscus can be injured by trauma or through a degenerative process. Sports injury accounts for most trauma-induced meniscal tears, usually from a bend-and-twist motion. Other injuries may be due to wear-and-tear of more brittle cartilage, a byproduct of the aging process. Often meniscal tears occur at the same time other components of the knee are injured. A common injury among athletes involves simultaneously the anterior cruciate ligament (ACL), the medial collateral ligament (MCL) and the meniscus.
In part due to the “C” shape of the meniscus, tears occur in a number of different locations. Flap, transverse, torn horn and bucket handle rank among the most common tears.
You may have heard a popping sound when your injury first occurred. After that, pain and swelling or tenderness may set in. Other symptoms include an inability to move your knee normally, or walk without pain or a clicking, uncomfortable feeling. For some, an injured knee may occasionally get stuck, or lock, at a 45° angle temporarily.
In order to diagnose you properly, your doctor will consider your symptoms, ask you about your activity leading up to the injury, and examine your knee carefully. Because meniscus injuries can also be accompanied by injuries to the other soft tissue in the knee, your doctor will want to look at the big picture. In addition to examining your knee in specific positions and manipulating its movement, your doctor will likely want you to have X-rays (to check for fractures) or an MRI (magnetic resonance imaging).